I know what you’re saying – what on earth is H. pylori infection and have I got it? I want to tell you a story of two amazing researchers who discovered why we get stomach ulcers and even proved it.
Trouble was, nobody would take any notice of them. Why? Because the powers that be and those that vetted all new research and cures, ignored their work. It went against everything previously taught. It was pure dogma and closed-mindedness. H. pylori stands for Helicobacter pylori a then unknown bacteria.
Dr Robin Warren
So who am I talking about? I’m speaking initially of Dr Robin Warren, a pathologist at the Royal Perth Hospital (RPH) in W. Australia. In 1979, he found evidence of bacteria in a stomach biopsy from a man with severe gastritis. Dr Warren was rather curious about this strange finding and a pattern began to show. Whenever there was chronic gastritis, the bacteria was present. He also noticed that the more inflammed the stomach lining was, the more abundant the bacteria.
Dr Barry Marshall

In 1981, Barry Marshall, who was in his second year of internal medicine, joined Dr Warren, in his investigation into the gastric spiral bacteria. Marshall’s interest was soon aroused. One of the patients was a woman he had seen on his ward. She had severe stomach pain but no diagnosis. She had been referred to a psychiatrist. Her prescription was antidepressents, for want of a better treatment. But she had some redness in the stomach. With a biopsy, Warren’s bacteria was found in her stomach.
No pre-conceived ideas
Warren had approached other colleagues to join him. But Marshall’s obvious advantage was that he had no pre-conceived ideas about the possibility of bacteria living in the acid-filled stomach. He did not come from a background of gastroenterology. His knowledge to that date was based on science rather than dogma which seems to be a requirement to learn specialist medicine.
Attempts at culturing H. pylori
In April of 1982, Warren and Marshall had attempted to culture samples from 30 patients but without success. During the Easter holidays, the hospital was fighting an outbreak of Staphylococcus aureus. Consequently, the latest culture attempt was left in the uncubator over the  holidays. It was normal procedure to leave the cultures to incubate for just two days, after which, if no growth was evident the cultures were discarded. When the staff came back after the holiday, they were surprised to find that the cultures were showing growth. It was then apparent that this spiral bacteria was a slow grower. For the previous 6 months, lab technicians were throwing away viable cultures after 2 days. This is the normal amount of time a culture is left to grow. It just shows how paradigms and habits can sometimes keep research blinkered.
holidays. It was normal procedure to leave the cultures to incubate for just two days, after which, if no growth was evident the cultures were discarded. When the staff came back after the holiday, they were surprised to find that the cultures were showing growth. It was then apparent that this spiral bacteria was a slow grower. For the previous 6 months, lab technicians were throwing away viable cultures after 2 days. This is the normal amount of time a culture is left to grow. It just shows how paradigms and habits can sometimes keep research blinkered.
Their research rejected
In July 1982, Marshall moved to Port Hedland Hospital, a position allocated to him within his training. Marshall used this time to do an extensive literature search and write up all the work they had done thus far ready for presentation. Warren and Marshall presented their findings to the College of Physicians at RPH in October 1982. Their work was not very well received.
Skepticism ruled
There was much skepticism and many objections one of which was the link between gastritis and duodenal ulcers. It was common knowledge that gastritis was associated with gastric ulcers but not duodenal ulcers. Marshall did some more research and found that there had already been evidence way back in the 1950’s. The Mayo Clinic carried out post- mortems on vehicle fatalities or partial gastrectomy patients. They were 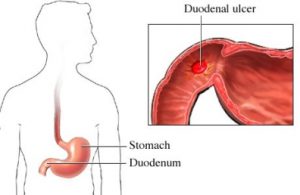 looking for the evidence of gastritis and ulcers. Those who had duodenal ulcers (N = 250) were all found to also have gastritis. This evidence way back in the 1950’s supported Warren and Marshall’s study. But still, the ulcer research fraternity ignored this relationship between gastritis and duodenal ulcers. Marshall speculated that their work was dismissed because it did not fit in with current beliefs and paradigms.
looking for the evidence of gastritis and ulcers. Those who had duodenal ulcers (N = 250) were all found to also have gastritis. This evidence way back in the 1950’s supported Warren and Marshall’s study. But still, the ulcer research fraternity ignored this relationship between gastritis and duodenal ulcers. Marshall speculated that their work was dismissed because it did not fit in with current beliefs and paradigms.
Marshall goes to Fremantle Hospital
He was then offered a position at Fremantle Hospital as a senior registrar with funding to continue the research. The smallest of teaching hospitals in Perth, Fremantle had a tradition of experimentation and open-mindedness and Marshall took up the offer. The only downside was that he was forced to finish his collaboration with Warren. Even so, Marshall was surrounded by an enthusiastic group of helpers at Fremantle. One of which was the pathologist Ross Glancy who joined the team.
The Bismuth Test
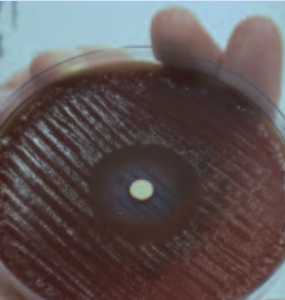
It was here that Marshall found out why ‘colloidal bismuth subcitrate’ (CBS) reduced the relapse rate of ulcers. He summised that CBS should have anti-microbial properties and he proceeded to test it. He soaked a filter paper disc in CBS and placed it in the middle of a Petri dish inoculated with H. pylori. After a few days and to his delight, there was a clear zone of inhibition around the paper disc.
In 1983 a Dr Martin Skirrow arranged for a presentation to be made to the European Campylobacter Meeting in September 1983. Marshall visited Dr Martin Skirrow in Worcester England. Dr Skirrow’s registrar successfully isolated the bacteria 3 days later.
Proof that organism was worldwide
This proved that the spiral organism was in fact worldwide and not just a product of Australia. Further proof came from several groups around the world who were also obtaining similar results. The European group came about from the campylobacter group Marshall had met in Brussels in 1983 and they were now a close knit community sharing and writing remarkable accounts of the research. This was to change the lives of millions of gastritis and ulcer sufferers.
Research still rejected!
1984 was a difficult year for Marshall. Most of his work was rejected for publication and the research was met with constant criticism. Marshall was disbelieved and the work was disputed, mainly on the premise that it simply could not possibly be true. Everyone knew nothing could live in the acid stomach. After all, it was written in the text books! This was despite the fact that patients were being treated and cured with a disease that many had suffered for years. For the treatment to be recognised and accepted within the medical community, Marshall had to come up with something radical.
Desperation!
 Out of desperation and frustration, he came up with the idea of infecting himself. His research had shown that H. pylori was sensitive to antibiotics. Marshall himself had successfully treated gastritis patients using antibiotics and bismuth. He isolated the culture he was to drink, from a patient with active gastritis. There was also an antibiotic available, metronidazole, which was effective in irradicating the cultured bacteria. The patient was then given a 2 week treatment of bismuth and metronidazole and was cured of the disease.
Out of desperation and frustration, he came up with the idea of infecting himself. His research had shown that H. pylori was sensitive to antibiotics. Marshall himself had successfully treated gastritis patients using antibiotics and bismuth. He isolated the culture he was to drink, from a patient with active gastritis. There was also an antibiotic available, metronidazole, which was effective in irradicating the cultured bacteria. The patient was then given a 2 week treatment of bismuth and metronidazole and was cured of the disease.
Marshall took Tagamet for one month
Marshall took an anti-acid drug known as cimetidine (Tagamet) for one month* before drinking the 3 day culture. Seven days later he became very ill and began to vomit. An endoscopic biopsy of his stomach showed, much to his relief and obvious satisfaction, that he indeed had gastritis with the presence of Helicobater pylori. Marshall began antibiotic treatment a few days later and his symptoms soon disappeared. Another endoscopy proved all traces of Helicobater pylori had gone. This was irrefutable evidence linking Helicobater pylori infection of a normal stomach to gastric inflammation.
Marshall returns to the Royal Perth
At the end of 1984 Marshall moved back to Royal Perth Hospital to conduct a double blind trial for antibiotics to see if they could cure duodenal ulcers. The Australian Medical Research Council was to fund the trail on the condition Marshall could enlist a large number of patients. He would be working with Robin Warren again along with other colleagues. He and Warren still kept in touch and discussed the papers they were writing for The Lancet. They would often meet for dinner with their wives. Marshall was anxious to share the news about his self experimentation and Warren was equally excited. Now they had first hand confirmation of infection and documented results.
Ignorant reporter!
At 5 am the next morning, Warren received a phone call from the USA. It was an inconsiderate journalist. He asked the usual stupid questions about the bacteria being just a harmless commensal and not a pathogen at all.
Warren loses his temper
Warren irritated, blurted out that they knew it was a pathogen because Barry Marshall had just infected himself and ‘damn near died’. The unreleased work was now in the hands of a journalist from the ‘Star’ tabloid newspaper. Freakish, bizarre and somewhat far-fetched copy was their speciality and this story was just up their street. The next day the ‘Star’ published “Guinea-pig doctor discovers new cure for ulcers…and the cause”.
As it happens, this unwanted publicity was to change Marshall’s life for the good and it was thanks to Warren’s temper. A continuous stream of patients from the USA had read the story and were desperate for the new treatment. Marshall was able to help these patients by proxy in the USA as early as 1984. This documented story and the subsequent records from the treated patients was also important. Another medic tried to claim credit for being the first discoverer. Marshall was able to prove his claim to be the first along with Warren.
Dogma kept patients in misery for years.
It wasn’t until 1994 and after many years of research that the medical community started to come around to the theory of bacterial infection and the consequence of ulcers. The medical profession had thought that peptic ulcer disease was caused by too much stomach acid. This fact was laid down in medical textbooks. Because of dogma, many long suffering patients tolerated untold misery and unpleasant surgery. Once a patient had an ulcer it was difficult to erradicate. Most kept their ulcers for life, controlling their flare-ups with drugs.
Intransigent medical community capitulate

How lucky it was that these two researchers were as tenacious as they were. One driven to putting his own life at risk to prove something that had already been proven. But despite this proof, it was not recognised or accepted by the medical fraternity. Unnecessary years of suffering had to be endured because of the pig-headedness of the medical community. Warren first was suspicious of this bacteria way back in 1979. If only the medical community had taken notice and started listening and upping the research. Then all those years of suffering and misery and death for so many patients, could have been avoided.
Marshall and Warren’s nobel prize speeches
In Barry Marshall’s nobel prize speech he mentioned that Warren’s wife had indicated in 1982 that there may be a nobel prize in the offing for this research. Marshall cynically replied that if so, it wouldn’t happen for ages, perhaps 1986. Dr Robin Warren and Dr Barry Marshall were jointly awarded the Nobel Prize for their research in 2005!
26 years of unnecessary suffering and death!
From 1979 – 2005. For 26 years patients were suffering, being operated on and dying needlessly, all because of medical dogma If anyone’s interested here’s a link to their nobel prize speeches:
http://www.nobelprize.org/mediaplayer/index.php?id=614 http://www.nobelprize.org/mediaplayer/index.php?id=616
 Why still PPIs? – pharma profits?- you bet!
Why still PPIs? – pharma profits?- you bet!
Out of curiosity, I had a little look around for the now known treatment of gastritis and/or ulcers. We already know that Marshall was treating and curing patients with ulcers way back in 1984. As Marshall himself writes: “I was successfully experimentally treating patients who had suffered with life threatening ulcer disease for years. Some of my patients had postponed surgery which became unnecessary after a simple 2 week course of antibiotics and bismuth”.
So why is it that patients with ulcers now, are still being treated with proton pump inhibitors such as Nexium. Why is the medical profession not using just antibiotics and bismuth as Marshall did way back in 1984? Could it be something to do with still pushing cimetidine and other money spinning PPI drugs?
* Marshall took an anti-acid drug known as cimetidine (Tagamet), a proton pump type inhibitor, for one month before drinking the H. pylori culture. Why? To stop his stomach from producing acid which would allow the bacteria to take hold. This proves that taking these drugs seriously impairs your capacity to digest and absorb nutrients because of induced low stomach acidity. It also suggests that low stomach acid, not excess acid, is the main  cause of digestive problems, which can lead to ulcers and cancer. See my previous post at https://magnesiumandhealth.com/proton-pump-inhibitors-side-effects/
cause of digestive problems, which can lead to ulcers and cancer. See my previous post at https://magnesiumandhealth.com/proton-pump-inhibitors-side-effects/
Spread the word!

I have just been diiagnosed with h pylori, i have just finished a 7 day course of Nexium HP 7 is this as the antibiotics you mentioned. Can you tell me what Bismuth is.??????
Thank you
Maryanne
Hi Maryanne, Nexium is not an antibiotic it is a proton pump inhibitor but you may have been prescribed antibiotics with the Nexium, these likely to be amoxycillin and clarithromycin. It is always advised never to take a PPI for more than 2 weeks because of addiction and the fact that stopping acid production is not good for you. The manufacturers of Nexium will deny it is addictive. Many who have taken it find it difficult to stop because when they do their symptoms come back with a vengeance making it necessary to start PPIs again to stop the recurring symptoms.
Gastric acid is important to breakdown your food and release the micronutrients. Some vital nutrients may be compromised because of the lack of acid. Low levels of magnesium (Mg) can be found in those taking PPIs. If you are already deplete in magnesium, the PPIs will definitely deplete your levels even more. Ask your doctor about taking a good quality Mg supplement but don’t hold your breath, most doctors don’t know about nutrients and can get testy if you challenge them about nutritional deficits due to drugs.
I am not a doctor, but if I were to take PPIs (which I wouldn’t) I would certainly up my intake of Mg to compensate for the depletion the PPIs would cause. But this is just my personal opinion. My post Proton Pump Inhibitors Side Effects will give you some idea of how these drugs work.
As for your question about Bismuth, ‘Colloidal bismuth subcitrate’ (CBS) reduces the relapse rate of ulcers according to research done by Dr Barry Marshall. He summised that CBS should have anti-microbial properties and he proceeded to test it. He soaked a filter paper disc in CBS and placed it in the middle of a Petri dish inoculated with H. pylori. After a few days and to his delight, there was a clear zone of inhibition around the paper disc. Good luck and I sincerely hope your symptoms improve but please do your own research, you will be amazed at what you can learn and there is no reason why you can’t be just as informed about your condition as your doctor is.
Hi Ches, thank you for sharing the information about H Pylori infection in your site. Normally, it would be very hard to stay focus on reading a medical related article because of the complicated not so easy to understand medical terms and jargon. However, I found your article very informative with very minimal technical medical jargon. In one of your response to the comments, you mentioned about calcium supplement. I am constantly having pain at my my finger both of my hands. Sometimes the pain moves from fingers to the wrist. Calcium supplement give me a pain relieves for a few days. I bought the calcium supplement over the counter, the pharmacist said that for this particular calcium supplement, I do not need a doctor’s prescription as it is natural herb type of calcium. In your opinion, should I stop the calcium supplement intake? For your information, I only took the calcium supplement occasionally. Thanks.
Hi there Juraida and thanks for reading my somewhat lengthy article. Your comment about medical terms and jargon was much appreciated as I do have concerns about being too technical or not technical enough. Over simplifying can sometimes compromise the information, but I don’t want readers ‘glazing over’. As for your wrist and finger pain, it may be a good exercise for you to work out your daily intake of Calcium (Ca). A daily allowance of 500-600mg is all that is needed for a healthy Ca intake. Unfortunately, we often consume twice, three times or more. Ca is in many foods so your intake can get into the thousands of milligrams without much effort. Food manufacturers also fortify many foods with Ca. At the same time, nobody mentions Magnesium (Mg) which is absolutely vital for our well-being and needs to be equal in intake to Ca ie a ratio of 1:1 Ca:Mg. If you know you are consuming more than 600mg of Ca per day, leave off the Ca supplement and start taking a good quality Mg supplement instead. Mg Chloride in liquid form such as ReMag or Ionic Mg is 100% bioavailable and is the best to take IMHO. Read the instructions on the bottle, one dose is 1/2 teaspoon or 2.5ml. Get up to at least 3 doses per day, starting slowly ie day 1 – 1 dose split into 2, then up the dose by half each day until you’re taking 3 doses. Always split your doses. If you have trouble sleeping make sure you have a dose before bedtime. Let me know how you get on and if you have any more questions, just leave a comment and I will answer. I am sure your condition will improve with Mg supplementation. Ches
PS take a look at this post it will give you an insight as to what too much Ca can do.
Chessie,
You are so right. I have never heard of this disease. I found it interesting. Fortunately, I do not suffer from ulcers or stomach problems. I do believe that the Drug companies don’t want us to know about simple solutions. They have too much money at stake.
Best wishes,
Joy
Thanks for the positive comments Joy. Ches
Wow thanks for this, there is so much quick and easy information for something I really had no idea about. It’s amazing what infections and diseases are out there and how hard it is to try and find a cure to help all of it.
Extremely well written too! Keep up the good work!
Kyle.
Thanks for the kind comments Kyle. Yes, there is much research to be done but at least those patients with ulcers and gastritis can now be cured and do not have to suffer their whole lives from a condition that was incurable a few decades ago. Ches
After reading your site I am going to look into buying this for me I’m always tired and have trouble falling asleep.The way your site is put together is very easy to read and understand. The writing flows from one paragraph to the next. Your site is perfect the way it is no need to change anything. The links work well, and the side panel works well also. Good job.
Thanks for the positive comments Charma and I’m pleased you’re going to try the magnesium. Please don’t buy the cheap magnesium oxide, it is not very bioavailable and will go straight through you. The best one to buy is magnesium chloride which comes in solution. ‘ReMag’ is probably is good but it is expensive and only available in the US. ‘Ionic Magnesium’ is just as good and a little cheaper and you can get that in the UK as well as the US. If you’re always tired and can’t sleep, this will definitely help you. Don’t drink milk or eat anything with a high calcium content before bed. If you’re taking calcium supplements, I would advise you to stop, unless they have been prescribed by your medic. Take a half dose of Mg chloride twice a day to start and gradually up your dose by half each day until you’re taking at least 300mg or more per day. Always split your doses. I keep a 1 litre (about 2 pints) jug of water on the side with the days amount in it (I take 600mg per day) and drink during the day with the highest amount for the evening before bed. Some dislike the taste, salty and bitter. Put a dash of cordial or juice in the water if you prefer. Good luck, good health and sweet dreams! Ches
Wow you learn something new everyday because your right, i have never heard of h pylori infection. The ulcer disease seems very dangerous and your writing is very personable as you use a lot of terminology which i dont know about. It certainly encourages me to learn more about this infection
Hi Jazzy and thanks for your comment. I sincerely hope the terminology is not too heavy going. It is difficult to keep to the point without losing important information. Many people will already have H. pylori in their gut. It’s when it migrates to the stomach that it becomes a problem. Try and avoid PPIs which are now available off the counter and don’t take antacids like ‘tums’. You must keep your stomach acid up. It is too little stomach acid that will cause digestive problems, very rarely is it too much. Good health always, Ches